My Profile
Homepage
Sign Out
Questionnaire
Home
Questionnaire
Submit Questionnaire
Are you sure you want to submit this questionnaire?
The questionnaire was submitted successfully and can be resubmitted after 2 weeks
The questionnaire data entered has incorrect or missing values
General Questionnaire
Gender
Select Gender
Male
Female
Age
Weight (Pounds)
Height (Feet)
Exercise Questionnaire
How do you rate your current level of fitness?
Select Fitness Level
Beginner
Intermediate
Advanced
Body Fat Percentage
Select Fat Percentage
──────────
Men
──────────
Under 8%
10-14%
15-18%
22-25%
Over 30%
──────────
Women
──────────
Under 15%
15-18%
19-22%
24-30%
Over 30%
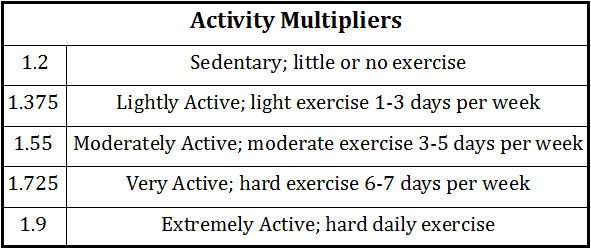
Activity Level
Select Activity Factor
1.2
1.375
1.55
1.725
1.9
Goal
Select Goal
Maintain Weight
Build Muscle
Cut
Recomposition (maintaining weight)
Do you have any physical limitations or medical conditions that may affect your workout?
What’s your short-term goal for the next 12 weeks?
Are you training consistently? What is your frequency?
When was the last time you were consistent and for how long?
What are your main motivations for wanting to lose weight or gain muscle?
Is there anything else you would like me to know when creating your workout program?
Fit Test
Can you touch your toes?
Select Answer
Not Even Close
Nearly
Just
Easily
If you went out for a jog, how far do you think you could go before you had to stop for a rest?
Select Answer
I wouldn't make it to the mailbox
To the end of the block
About a kilometer or mile
A long way
How would you describe your push-up ability?
Select Answer
I am a beginner (0-10 push-ups)
I am building strength (10-20 push-ups)
I am in good shape (30 or more push-ups)
How would you handle the task of moving heavy items around the house? (e.g., Couches, refrigerator, etc.)
Select Answer
I would be no help
I would pitch in but need a few helpers
I could carry one end of it myself
I could possibly do it myself
What could you jump over?
Select Answer
A small box
A medium box
A large box
Nutrition Questionnaire
Have you ever followed a specific diet before? If so, what was it and how successful were you?
If you keep on failing to commit to a diet plan, explain why?
Do you have any dietary restrictions or allergies?
How many hours of sleep do you get each night?
How much water bottles do you drink per day?
How many meals per day do you typically eat?
Select Number of Meals
1
2
3
4
5
6
Fitness Journey Assessment
What are your biggest obstacles or challenges when it comes to losing weight or gaining muscle?
What is your biggest struggle in seeing results?
How long has that been a problem?
What have you done to fix the problem?
Has that worked for you, If yes for how long?
Save Changes